
A ‘dorsal hump deformity’ refers to an undesirable bump involving the bridge, or dorsum. This is best appreciated on the lateral view of the nose and appears as a convexity over the bridge (see photo example). In some cases, a dorsal hump deformity is barely noticeable on frontal view. Most patients present stating they often see the unwanted bump in photographs of themselves taken from an oblique, or partial side, angle.
Esthetic Analysis and Goals
Rhinoplasty patients with a dorsal hump deformity usually request changes that will result in a straighter, smoother bridge as seen on lateral view. However, there are various degrees of ‘straighter’ when discussing rhinoplasty for a hump deformity. The most often requested change to a dorsal hump is to provide a straight bridge as seen on profile view. This can be done with or without what is termed a ‘supra-tip break’ (also known simply as a ‘tip break’). A supra-tip break refers to a slight angulation, or break, in an upward direction as the bridge junctions with the tip (red arrow in attached photo). This results in the tip being 1-2 millimeters higher than the remainder of the bridge. This is often considered a feminizing trait and should be avoided in the male nose.
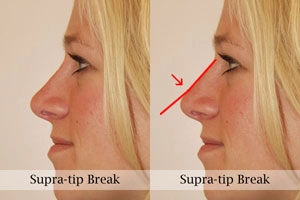
Dorsal hump removal can also be done without leaving a supra-tip break while still achieving an esthetically pleasing profile. For example, the adjacent photo of a Dr. Hilinski patient demonstrates removal of a hump deformity without leaving a supra-tip break. The end result is an essentially straight bridge while maintaining a natural, balanced profile view. The decision to leave a supra-tip break or not is very much an individual one that should be discussed and reviewed in detail with Dr. Hilinski during your consultation.
A nasal profile with a supra-tip break should not be mistaken with the scooped, or ski slope, bridge that was popularized in the 1970s. Whereas the supra-tip break reflects a slight shift in direction, the scooped bridge is more of a continuous curve extending from the upper bridge to the tip (resembling a ski slope). The attached photo (prior rhinoplasty performed by another plastic surgeon) visually demonstrates this undesirable contour, which carries with it an obvious stigma of having overaggressive surgical removal of a hump.
In recent years, my practice has seen an increasing number of rhinoplasty patients who are now requesting partial hump removal. Instead of desiring simply a straight profile view, these patients aim to have their hump altered while leaving a residual bump, or convexity. This is most often done in patients who are looking to have their nose reshaped while preserving more of their ethnic identity, which sometimes emanates from the nasal dorsum. In fact, I have now revised several rhinoplasty patients who had surgery elsewhere and desired at least partial replacement of the bump that was originally removed.
Surgery for A Dorsal Hump Deformity
Surgery to remove a dorsal hump deformity is often described as a ‘reductive’ rhinoplasty since it results in a reduction in the size of the nose. By definition, reductive rhinoplasty involves removal of a certain amount of cartilage and/or bone to achieve the desired appearance. Contrary to popular belief, this is actually one of the most challenging types of rhinoplasty to perform while achieving successful long-term results . This is largely due to the fact that changes involving the middle one-third of the nose (see section on Nasal Analysis), where most bumps exist, can significantly alter the three-dimensional appearance of the nose. It is relatively easy to reduce a hump deformity and achieve acceptable esthetic results as seen from the two-dimensional profile view. It is much more difficult, however, to achieve proper symmetry and balance of the bridge from all three views (profile, oblique and frontal) following hump reduction. This is precisely why many plastic surgeons will often publish only the profile view of their hump reduction patients.
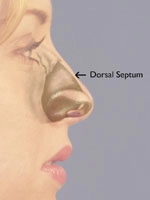
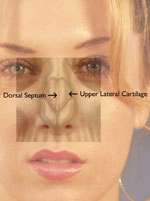
The challenge in achieving excellent results in three dimensions is based on the underlying anatomy. The middle one-third of the nose is comprised of the dorsal septum with the upper lateral cartilage on each side (see adjacent diagrams). Together, these structures form the support for the middle one-third of the bridge and play a key role in the appearance of the mid-dorsum. This is a critical anatomic relationship that if compromised during hump reduction can eventually lead to unwanted collapse of the upper lateral cartilages. This is a complication that may not be noticed during the first 6-9 months following surgery because persistent swelling of the overlying tissue helps to camouflage the deformity. As time goes on, however, the middle one-third of nose begins to pinch inward, leaving a noticeable inverted V-shaped shadow across the bridge (also known as an inverted V deformity). Such a deformity significantly disrupts the brow-tip esthetic line (as discussed in the Nasal Analysis section) and brings unwanted attention to the area. Prevention of this complication relies on careful preoperative planning and meticulous surgical technique. Thus, Dr. Hilinski may recommend use of cartilage grafts (termed spreader grafts) as part of your dorsal hump reduction procedure. Placement of such grafts helps to stabilize the integrity of the mid-dorsum and increases chances of having a smooth bridge once complete healing has taken place.
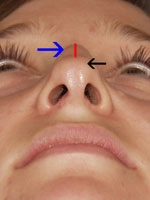
In addition to these concerns, the nasal bones, or nasal vault, (see discussion in Nasal Analysis section) must be assessed during hump reduction. In most cases where at least a moderate reduction is being performed, the nasal bones also need to be narrowed. This requires what is termed an osteotomy, which means cutting the bone. In layman’s terms, this is breaking the bone. If this is not done when indicated following hump reduction, the nasal bridge may appear excessively wide from the frontal view. The adjacent diagrams are provided to illustrate this point. The diagram on the left demonstrates how high (red line) a dorsal hump deformity (blue arrow) might rise above the level of the nasal tip (black arrow). The diagram on the right demonstrates how much the nose may be effectively widened after reducing the bridge height by this amount (compare red and blue lines). Osteotomies are performed to compensate for this potential by narrowing the bridge to a more appropriate width.
In addition to the esthetic challenges, there are key functional considerations with dorsal hump reduction. The previously mentioned dorsal septum and upper lateral cartilage form an anatomic angle on the inside of each nasal passage, termed the internal nasal valve. This angle happens to be the area of the nasal passage that has the highest resistance to airflow. Consequently, even subtle narrowing of the internal nasal valve can result in subjective feelings of difficulty breathing through the nose. In cases where the upper lateral cartilage is excessively long (and the nasal vault is short) there is a higher likelihood of causing internal valve collapse by dorsal hump reduction. In these cases, it is often recommended that spreader grafts be placed to help restore and reinforce the integrity of the internal nasal valve. In this manner, there is less chance for compromised nasal breathing following surgery. In cases where the upper lateral cartilage is relatively short (and the nasal vault is long), it is usually not necessary to place spreader grafts, as there is less likelihood of causing narrowing of the internal nasal valve region.
In summary, dorsal hump reduction is one of the most challenging types of rhinoplasty given the fact that changes in the middle one-third can significantly impact the three-dimensional appearance of the nose. In addition to the esthetic considerations, one must also pay close attention to the functional implications of altering this region of the nose. This may include likely osteotomies and possible placement of spreader grafts once the hump has been reduced. With thorough preoperative planning and proper surgical technique, one can help maximize chances of achieving an esthetically pleasing result while maintaining optimal nasal function.