A saddle nose deformity refers to a marked depression or collapse along the mid portion of the nasal bridge. It is described as such because it resembles the look of a saddle when looking at the nose from the side view. This is visually demonstrated in the adjacent diagram showing precisely where the nose collapses in most cases of a saddle nose deformity. Because of the appearance, this type of abnormality has been also referred to as a ‘pug nose’ or ‘boxer’s nose’ deformity.
What Causes A Saddle Nose?
A saddle nose deformity can be caused by a variety of factors.
In some cases, a saddle nose deformity can arise from an underlying medical condition that affects the cartilage structure of the nose. These include Wegener’s granulomatosis, leprosy (also known as Hansen’s disease), relapsing polychondritis, and even syphilis. With each of these medical conditions, the end result is severe damage to the cartilage structure of the nose with subsequent collapse of the nasal bridge. Fortunately, these medical diseases are quite rare overall and account for a minority of saddle nose deformities.
A majority of saddle nose deformities result from prior trauma to the nose. This can be from previous nose surgery (yes – nose surgery can be traumatic) or an actually injury to the nose (such as a boxer or mixed martial artist getting punched). Saddle nose deformity as a result of prior nose surgery can arise if excess cartilage is inadvertently removed from the nose. This happens most commonly when a rhinoplasty surgeon reduces the bridge height by an excessive amount. In this particular case of a saddle nose deformity, the nasal bone, dorsal cartilage and/or upper lateral cartilage can be compromised to the point where there is insufficient structural support to maintain proper bridge height. The result is collapse of the nasal bridge through the mid portion as seen on profile view. This same thing can result when someone suffers blunt trauma to the nose, such as a boxer. In this type of saddle nose deformity, it is usually the septal cartilage that becomes damaged and weakened. Consequently, the bridge support is compromised (as is seen with surgical trauma), resulting in a saddle nose deformity. In either case (saddle nose following surgery or trauma), the bone and/or cartilage support of the nasal bridge is damaged to the point of causing a collapse.
Saddle Nose Deformity Presentation
There is actually a grading system developed to rate the severity of a saddle nose deformity. However, in most rhinoplasty practices, they are basically two types of saddle nose presentation – one that involves only the nasal bridge and the other that also involves changes to the nasal tip as well as the bridge.
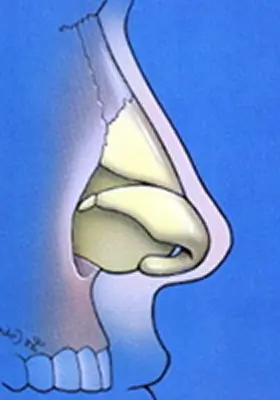
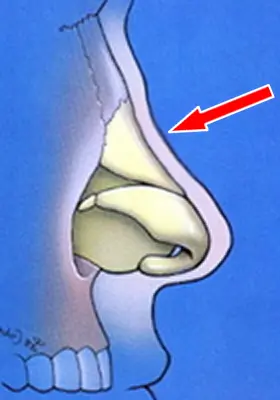
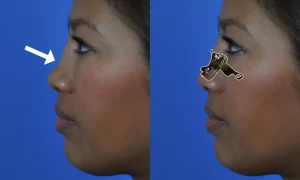
The first type of saddle nose deformity involving only the nasal bridge is depicted in the adjacent diagrams where the left side is normal. On the right you can see the red arrow showing how the bridge cartilage collapses and the overlying soft tissue essentially sinks inward leaving a saddle deformity. As is shown, the nasal bone can be involved in many cases as it junctions with the upper lateral cartilage and dorsal septum. All three of these anatomical structures can collapse leaving the bridge with a saddle deformity. A real patient example of this type of saddle nose deformity was shown above at the start of the discussion.
In the second type of saddle nose deformity, the nasal tip is affected along with the bridge. Like the first type of saddle deformity, the nasal bridge collapses inward due to compromise of the nasal bone, upper lateral cartilage and dorsal septum. However, in this type of saddle deformity the damage to the bridge cartilage is so severe the adjacent tip cartilage is also affected. In this situation, scarring begins to affect the nasal tip, which starts to rotate upward in an abnormal fashion. This means the nasal tip begins to look too short – similar to a pig nose deformity. In fact, this is largely why a saddle nose deformity has also been described as a pug or boxer’s nose as seen on profile view.


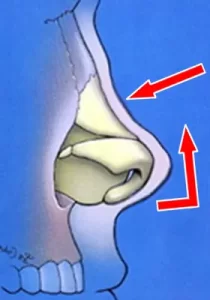
This concept is demonstrated in the adjacent diagram showing how the nasal bridge can collapse while the nasal tip rotates upward (two red arrows showing the direction of change seen in this type of saddle nose deformity). Compare this diagram with the one shown above without any nasal tip alteration. You can see in this second type of saddle nose deformity that the lower lateral cartilage is displaced from its normal position, causing the nasal tip to rotate upward. The adjacent patient examples show this type of saddle nose deformity where the bridge has collapsed and the nasal tip has rotated upward at the same time.
On frontal view, a saddle nose deformity appears too flat and wide across the area where the bridge is collapsed. This is because the depression creates unwanted shadowing in between areas of the nose that have maintained proper height (namely the upper bridge and tip). This is analogous to looking at an aerial view of the Grand Canyon, for instance. The river flowing through the canyon is like the saddle deformity where collapse has occurred. In contrast to the surrounding rim of land, there is an obvious shadowing effect that can be seen because the canyon floor is much lower. You can imagine there would not even be a shadow if the land were the same height all the way across.

The adjacent photo example of the same female rhinoplasty patient featured above demonstrates this point precisely. As is indicated by the shaded trapezoid, you can appreciate that this area of her nose where it is saddled appears flatter and wider than desired. It also shadows more across the nasal bridge where the saddle deformity exists. On frontal view, this type of deformity will cause a significant disruption of the brow-tip esthetic line, which detracts from the ideal appearance of the nose.

The adjacent male rhinoplasty patient is another good example visually demonstrating what a saddle nose deformity looks like on frontal view. This patient, also shown above, has an even more dramatic saddle deformity with more severe flattening of the nasal bridge. This patient suffered a traumatic blow to the nose that resulted in collapse of both the bone and cartilage along the bridge area. This caused a severe saddle nose deformity, which was accompanied by distortion of his nasal tip. As the bridge began to collapse, the associated scarring, in combination with lack of cartilage support, lead to abnormal displacement and rotation of the nasal tip.
Surgery For Saddle Nose Deformity
Correction of a saddle nose deformity involves fairly complex rhinoplasty or revision rhinoplasty technique. Thus, this type of cosmetic nose reshaping should only be performed by a facial plastic surgeon who is well versed in advanced rhinoplasty procedures.
The most important goal in correcting a saddle nose deformity is restoring proper bridge support. In many cases, this involves reconstruction of the nasal bone as well as the bridge cartilage (dorsal septal cartilage and upper lateral cartilage). In nearly all cases of a saddle nose deformity, surgical correction will involve some form of augmentation of the nasal bridge. This means that something has to be added to the nose to help restore proper shape and support.
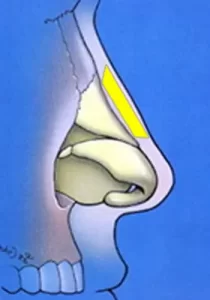
The most common technique used in my rhinoplasty practice to correct a saddle nose deformity is cartilage grafting. In some cases of a mild saddle nose deformity, septal or ear cartilage grafting may be sufficient to rebuild the nasal bridge. This is shown in the adjacent diagram and indicated by the yellow shaded area corresponding to a cartilage graft. In this type of rhinoplasty for a saddle nose deformity where the tip is not involved, a segment of cartilage can be placed directly over the depression to restore a normal bridge height. This is commonly referred to as ‘dorsal augmentation’ since the bridge of the nose is being elevated or built up. It is also known as a ‘dorsal onlay graft’ because the cartilage is being gently placed on the bridge to overlay the defect. Because the area that requires elevation is fairly limited, septal or ear cartilage is sufficient when reshaping this type of saddle nose.
In rhinoplasty patients who have a saddle nose deformity that also involves abnormal rotation of the nasal tip, more extensive cartilage is necessary to achieve a natural looking nose. In these rhinoplasty patients septal and/or ear cartilage is usually not strong enough for the reconstruction. In addition, this type of saddle nose deformity repair typically requires a larger graft than is available from the septum and ear. With this type of saddle nose correction, the bridge has to be augmented as noted above. However, the graft used to build up the bridge has to be longer to accommodate the more extensive saddle deformity seen in these patients.
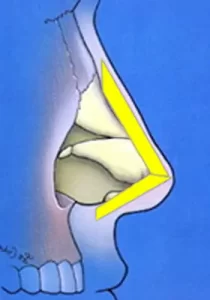
Furthermore, the tip also has to be reconstructed by lengthening the nose back to its original position. In this rhinoplasty population rib grafting (also known as costal cartilage grafting) is usually necessary to provide sufficient amounts of a resilient cartilage that will maintain proper strength and shape over time. This concept is shown in the adjacent diagram where you can appreciate how much more cartilage grafting is often necessary in this type of saddle nose correction. For instance, the dorsal onlay graft in this case is much longer and needs to often times extend into the nasal tip region in order to help reposition the tip. You can also see a second cartilage graft that is frequently placed under the nasal tip to provide further support for the reconstruction.
Many rhinoplasty patients with a saddle nose deformity inquire about other types of material that can be used to reconstruct the nose besides cartilage. Although there are other biocompatible materials, such as goretex, porex and silicone implants, I prefer to avoid these if cartilage grafting is a viable option. And even in cases where these types of nasal implants are used, they should only be placed overlying the bridge and must be avoided in the nasal tip region.
Nasal Obstruction And A Saddle Nose Deformity
A significant number of patients with a saddle nose deformity also note subjective feelings of nasal obstruction, or difficulty breathing through the nose. This is not surprising given the area of collapse involves the internal nasal valve (middle vault). To read more about the internal nasal valve and its implications in nasal breathing, please refer to our rhinoplasty tutorial chapter on middle vault reconstruction using spreader grafts. In a good majority of patients undergoing surgical reconstruction for a saddle nose deformity, there is passive improvement in their nasal breathing following the procedure. And this is without placement of spreader grafting. This is most likely due to the fact that re-elevating the bridge height helps to reopen the internal nasal valve much like popping up a collapsed tent.
Correction Of Saddle Nose Deformity
These photos here show how the above mentioned techniques can be used successfully to correct a saddle nose deformity.
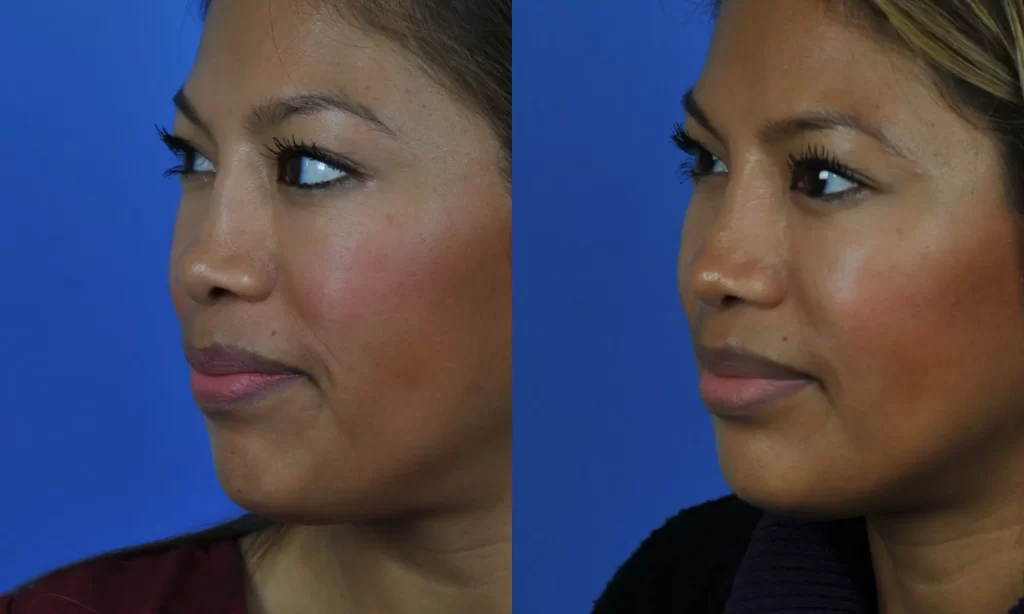
This first example was done using a closed rhinoplasty technique where cartilage grafts were used as described above to augment, or build-up, the bridge height. As you can see, she now has a more favorable appearing nose as seen from all three standard angles.


This second example demonstrates use of an open rhinoplasty technique where the bridge and the nasal tip were reconstructed concurrently to restore proper support. As you can readily see, there is a marked improvement in terms of the previously collapsed nasal bridge. There is also better nasal tip support. These anatomical alterations translate into a bridge and nasal tip that now look much more natural and harmonious with his face.



Saddle Nose Rhinoplasty Consult
If you have a saddle nose deformity and are considering rhinoplasty repair of your nose, do not hesitate in contacting our office today to discuss your concerns with one of regions best nose surgeons.