One of the more challenging types of reconstructive rhinoplasty involves repair of a caudal septum deviation.
Caudal Septum
So what is the caudal septum you might ask? The caudal septum refers to the portion of the nasal septum that sits right behind the columella – which is the column that separates the two nostril openings. The caudal septum can also refer to the anterior most segment of the nasal septum – meaning the segment that is closest to the bottom of the nose.
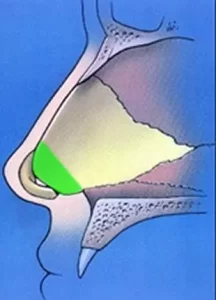
The caudal septum is shown diagrammatically in the adjacent image and is indicated by the green shaded area. The slightly curved segment of cartilage right in front of the shaded green area corresponds to one of the medial crura. Both medial crura attach very closely to the caudal septum and are important in determining the location and position of the actual nasal tip.
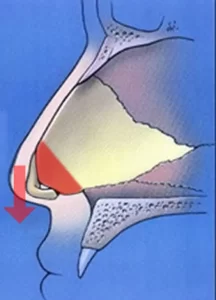
So what is the big deal about the caudal septum? Because it is so critical in helping to support the nasal tip cartilage, it is vital that rhinoplasty surgeons be mindful of the caudal septum. For example, if the caudal septum is removed, or resected, the medial crura cannot be adequately supported. Therefore, the medial crura essentially fall down. This then compromises the support of the entire nasal tip. In most cases, the nasal tip will droop down, or drop, if the caudal septum support is not sufficient. This is shown in the adjacent diagram as indicated by the red arrow.
In other cases, a compromised caudal septum will result in severe nostril asymmetry since the medial crura are not attached to anything that is supportive. This will lead to subjective difficulty breathing through the nose as the airway becomes blocked on one or both sides.
A Deviated Caudal Septum

This case example highlights the importance of the caudal septum and the need to find a qualified surgeon in San Diego that has knowledge and experience in correcting a deviated caudal septum. This male patient presented to Dr. Hilinski noting trouble breathing through his nose. On examination it was quite clear why he was having nasal obstruction.

You can see in the adjacent photo of the patient from below just how abnormal his nostrils are in terms of shape and size. Particularly on the patient’s left side (right side in the photo), you can see how much blockage there is in terms of airflow. When the patient pulls the tip slightly over to the side, you can see even more readily how much nasal blockage there is on that side. In fact, he has barely a ‘slit-like’ opening to breathe on his left side.
This is all primarily due to an abnormality with his caudal septum. Facial plastic surgeons and rhinoplasty surgeons would also refer to this as a deviated caudal septum, a displaced caudal septum and a caudal septum deformity. No matter how you label it, there is an anatomical problem with how the caudal septum is shaped and positioned.
Exposing the Caudal Septum
It was recommended by Dr. Hilinski that he undergo a complex nasal reconstruction using an open rhinoplasty approach. This was going to be the best way to expose all the pertinent anatomy in the region of the caudal septum. It was also going to allow Dr. Hilinski prime exposure for repairing the caudal septum with planned cartilage grafting.
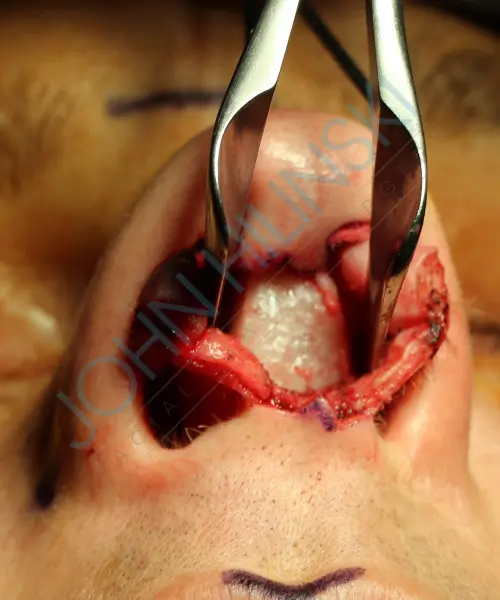
Here attached are several intraoperative photographs from this patient’s actual reconstructive septorhinoplasty surgery. The adjacent base view is taken from a similar angle as the clinical photos shown above. The metal nasal speculum can be seen spreading the paired medial crura apart to help expose the caudal septum as seen from below. A well-trained rhinoplasty surgeon would be able to see immediately just how abnormal this caudal septum is compared to a normal nose. Normally, one would see just the thin edge or end of the caudal septum. In this case, the caudal septum was so severely bent, it looked like Dr. Hilinski was staring at a wall.
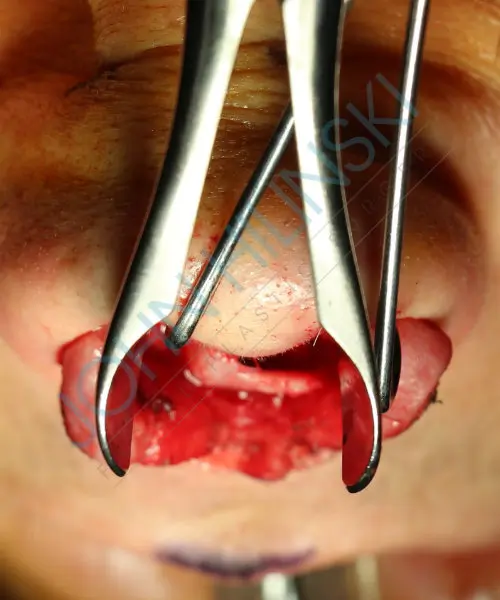
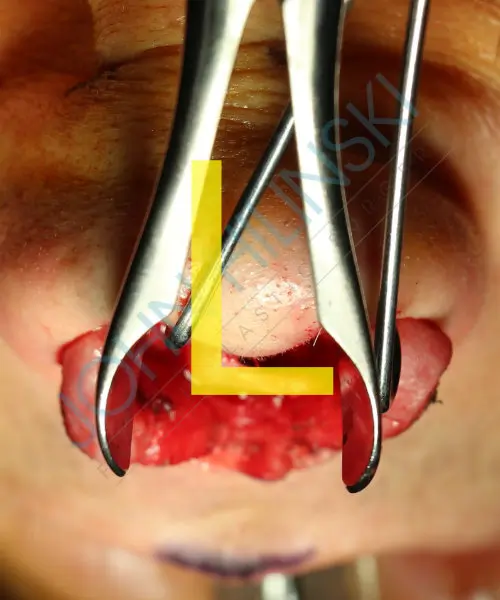
When this area of the caudal septum was then viewed from above – called the aerial view in rhinoplasty – you could see even more readily what the problem was with his nose. As the nasal speculum spreads the medial crura apart, you can appreciate how his caudal septum was actually forming a right angle! This is indicated by the superimposed ‘L’ as shown here. In fact, rhinoplasty surgeons will sometimes refer to this type of severe caudal deviation as being an L-shaped deflection of the caudal septum. But now you can see how and why this patient’s caudal septum was so displaced as to cause him severe trouble breathing through his nose.
Repairing the Caudal Septum
In this type of septal deviation, a surgeon cannot simply cut out the displaced cartilage. Why? Because we mentioned above how critical the caudal septum is to proper nasal tip support. If the caudal septum was just cut out and nothing else was done, his nasal tip wouldn’t have anything to properly support it – leading to collapse of the nasal tip after surgery.
In order to adequately and reliably address the caudal septum deviation shown above, Dr. Hilinski had to remove the deviation – but he had to replace this segment with a straighter piece of cartilage that could then proper nasal tip support. This is NOT your routine type of septoplasty surgery. This type of septal reconstruction is something that only true experts in septoplasty and rhinoplasty are trained to do. Meaning, most ENT surgeons in San Diego would not feel comfortable performing this type of septoplasty. That is why so many San Diego ENT doctors refer this type of septoplasty to an expert septal surgeon like Dr. Hilinski.

This type of septoplasty surgery is termed a subtotal septal resection procedure – since nearly all of the septal cartilage has to be removed before the caudal septum is reconstructed or repaired. The actual cartilage that was removed from this patient is shown here in the adjacent photo taken during his surgery. As you can see – now in all of its glory – the cartilage was indeed quite deviated. Why is the deviation not at a 90 degree angle as it was while in the nose? This is because the cartilage was attached to surrounding structures inside of the nose. Once the cartilage was removed, there was some relaxation noted.
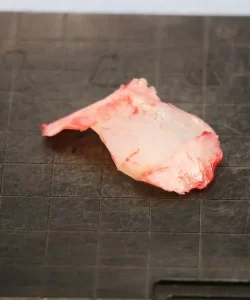
So how did Dr. Hilinski go about repairing the caudal septum? If you look at the rest of the cartilage taken out along with the caudal deviation, there was plenty of viable, straight cartilage behind it. This is seen here in the adjacent photo to the right. You can actually see the L-shaped displacement – along with the remainder of the cartilage harvested with it. Again, this is not the type of cartilage harvesting that is usually seen with routine, traditional septoplasty surgery performed by ENT surgeons. But that is another reason why this type of septal reconstruction surgery is only performed by specialists such as Dr. Hilinski.

Ultimately, Dr. Hilinski ended up using this other segment of cartilage to help rebuild a new nasal tip support mechanism. What this means is that Dr. Hilinski made a new caudal septum from this harvested septal cartilage and attached it to the nose. In doing so, he was able to replace the L-shaped deviation with a solid, straight, supportive new caudal septum. This new caudal septum is shown in the adjacent photo of this patient taken during surgery. Whereas his caudal septum was previously angled off 90 degrees as shown above – it is now appropriately positioned and shaped – coming straight out of the photo right at you. The cartilage was sewn to the surrounding cartilage and bone – and would eventually scar into place long-term.
The medial crura would then be sewn to the new caudal septum so that the proper tip position could be established. Now that the caudal septum has been correctly repaired by Dr. Hilinski, the nostril openings should be much more symmetrical. In turn, there should be a much better nasal airway on both sides – leading to a marked improvement in subjective breathing for this patient.
Before & After Caudal Septum Repair
Here are stable results showing before and after photos following repair of the caudal septum deformity in this patient. As you can see, Dr. Hilinski was quite successful in repairing the structural abnormalities noted above. In fact, the patient’s nostrils are now about as symmetrical as they come in terms of rhinoplasty reconstruction. This translated into a marked improvement in nasal breathing for this very fortunate rhinoplasty patient from San Diego. And as can be seen in his frontal views, his nose also looks aesthetically much better as a result of Dr. Hilinski’s surgery.



